

An art installation depicting the nuns to whom St. Joseph Hospital and Providence attribute their namesake, with a modified COVID-19 patient room can be seen from the sidewalk, with plywood and ducting visible in the background. [Photo by Ryan Hutson taken August 17]
Staff at Eureka’s St. Joseph Hospital tell us the ICU is struggling through the current surge in COVID patients with no beds available and a lack of high acuity equipment to meet urgent needs, especially in the Emergency Department. In the Intensive Care Unit where COVID-19 cases are far outnumbering staff, they are operating in “crisis mode,” according to those we interviewed.
One frustrated employee explained, “All the beds are taken. They’re talking about converting the PACU – post anesthesia care unit – into a secondary ICU because people are unvaccinated monsters!”
A nurse told us. “We are doing our best and our team is tired. They are just done.” The hospital is stretched thin to the point of having borrowed beds recently from Santa Rosa, and it recently had to make temporary modifications to rooms for COVID patients just to keep up.
This is unsurprising when taking into account the grim synopsis delivered to the Board of Supervisors last week from Humboldt County’s Public Health Officer Dr. Ian Hoffman. Confirming that the hospital and all others within Humboldt County had been at 100% capacity for “most of the past two weeks”, Hoffman also mentioned that several patients are being flown out of the area for treatment due to a lack of services available in Humboldt. Hoffman’s written update to the board stated in part, that the County’s ICU capacity “continues to be half or more COVID-19 patients, and has thus resulted in cancellation of many needed procedures that were deemed not emergencies… .” Hoffman clarified, “[T]he types of care that become deferred by the hospital during a surge of this type include things such as heart surgeries, cancer surgeries, joint and back surgeries.”
Another worrisome sign Hoffman noted was an increasing “trend toward younger and younger hospitalizations, likely since this is the group with the lowest vaccination rates in our county.”
As the flow of COVID-19 positive patients continues, nurses and staff at the hospital in Eureka are scrambling at times to accommodate the influx, on top of the normally full-throttle daily routine of caregivers at St. Joseph Hospital, the concentrated area where COVID-19 beds were arranged has sprawled out into various departments of the hospital campus. Currently, according to sources working directly with COVID-19 patients, they are putting them wherever there is an open room. It is all hands on deck, including the engineering team, as the COVID cases keep coming.
When we inquired with caregivers about how exactly the patients are being cared for in surge times, the consensus was that the hospital is doing it’s best to comply with Cal-OSHA standards requiring negative pressure airflow and HEPA filtration, effectively isolating patients in regular rooms, that are modified to conform to COVID-19 care standards. As one employee put it, “Those Covid patients are scattered around the hospital like chocolate chips in a cookie. That is unacceptable. We need some designated areas. We need to upstaff to take appropriate care of these patients just because of the time consumption that is involved.”
![<a href="https://kymkemp.com/2021/08/25/anti-mandate-rally-protesters-displayed-un-vaccinated-star-of-david-pins-during-controversial-protest-on-sunday/239532826_262242348874854_7539505859675053748_n/" rel="attachment wp-att-303051"><img class="size-full wp-image-303051" src="https://kymkemp.com/wp-content/uploads/2021/08/239532826_262242348874854_7539505859675053748_n.jpg" alt="An art installation depicting the nuns to whom St. Joseph Hospital and Providence attribute their namesake, a modified COVID-19 patient room can be seen from the sidewalk, with plywood and ducting visible in the background. Photo by Ryan Hutson, August 17th. " width="800" height="600" /></a> <em><strong>An art installation depicting the nuns to whom St. Joseph Hospital and Providence attribute their namesake, with a modified COVID-19 patient room can be seen from the sidewalk, with plywood and ducting visible in the background. [Photo by Ryan Hutson taken August 17]</strong></em>](https://kymkemp.com/wp-content/uploads/2021/08/237186692_563357848046973_5831364895639979976_n-1.jpg)
Rows of modified COVID-19 patient rooms with plywood and ducting visible can be seen from the outside of St. Joseph Hospital in Eureka. [Photo by Ryan Hutson]
The staff say they are overwhelmed in their various assignments on a day to day basis. The increased time and use of equipment needed to care for these COVID-19 infected patients is exhausting caregivers as well as resources and beds.
“When you have this many patients all at once, all across the County,…there’s no plan that can plan adequately for that. It’s a difficult job, and it’s one that we don’t want to be in…[V]accination could have prevented this.” said Humboldt County’s Public Health Officer Dr. Ian Hoffman today.
Last week, before the ICU reached full capacity, a staff member told us that COVID patients are also in the relatively new IMCU. “They increased the spillover from the ICU into the IMCU, the first three rooms are Covid rooms right now,” they explained… “So it looks like there are six patients in the ICU, but there are three more in the IMCU (Intermediate Care Unit) which is covered by ICU staff.”
When a person comes to the hospital needing COVID-19 care, if they are admitted, depending on the severity of their situation, they may be placed in an ICU isolation room, or in the Progressive Care Unit (PCU), or in the Intermediate Care Unit (IMCU), or in any room available that can be modified by the hospital’s engineering department into an isolation room with negative air flow.
While it is clear that these patients are situated according to their needs, the hospital is struggling to make space, according to multiple sources. One staff member who works with COVID patients regularly explained, “In regards to how they are housing Covid patients now, it’s called the RCU, they took it down back in the end of June, beginning of July and started integrating patients into just regular isolation rooms.”
These hospital-hacked COVID rooms are visible from the parking lot, and some from the street, identifiable because of their plywood installation and circular vent cutout in the window. These are likely occupied due to the current capacity level, but we are told that the windows remain modified for future COVID-19 care, after a patient recovers or (in some cases) expires.
A text received by our reporter from within the ICU confirmed for us Friday, August 20, that all of St. Joseph Hospital’s 12 ICU beds as well as several more in the ‘spillover’ Intermediate Care Unit were occupied with COVID patients. One employee, who says they are frequently stretched thin to the point of having to miss breaks and work overtime, was adamant that an emergency plan needed to be discussed in order to address immediate concerns about patient care and safety. “What is the emergency step plan for this surge?” they asked.
In a virtual Press Conference this morning, Dr. Hoffman confirmed that six patients have been transferred to neighboring area hospitals due to lack of beds available. He also mentioned that the hospital has negotiated a deal with the state to acquire additional staff to assist locally with the ongoing surge of unvaccinated infections.
Hoffman was not able to offer any details as to how many additional nurses or staff would be made available, but indicated he was hopeful that help would be arriving soon. While the struggle continues in real time at the ER in Eureka, Dr. Hoffman noted that the overflow site previously set up at Redwood Acres was dismantled due to lack of staffing available to work the site. Beds must be staffed accordingly, and without personnel, there can be no services provided.
Hoffman told our reporter, “Many many have retired from the stress of this pandemic. The extraordinary toll it takes to care for COVID patients has forced early retirement on many nurses.” He added, “So with this current surge, given the current numbers we’re seeing, we’re competing against – not just our local counties that are surging worse than us, like Del Norte…”
Alluding to a decision to expand ICU capacity locally, Hoffman was hopeful that when additional ER staffing arrives, those additional beds will ease the strain of resources.
At the time of publishing, there are 33 currently hospitalized [updated at 1 p.m.] with COVID in the County, and 11 of those are noted in the ICU. To date, 65 county residents have died from the infection. Between August 7 – 13, Humboldt County added 30 hospitalizations for COVID-19 county-wide, and counted an additional 2 deaths that week. Last week was similar, counting 29 added to hospital beds, and 4 lives lost between August 14 – 22 and three dead in yesterday’s count alone..

California’s hospitalization data shows that St. Joseph Hospital counted 15 COVID-19 patients in ICU care on August 19, 2021, when the ICU hit full capacity in Eureka. Several sources confirmed for the Redheaded Blackbelt that the Emergency Department recently has not been able to process patients in a timely way, at times causing next-day waits for people needing attention, and even turning away people who would otherwise have been admitted for care, but could not be tended to at the time they arrived. One staff member woefully explained that standards of care are simply not able to be met under the current surge circumstances.
We were told, “The staffing situation is so bad right now that there are COVID-positive patients that, ordinarily, if somebody came into the hospital with the symptoms that they have, they would be admitted because that’s what we have to do, but instead because of our bed limitations we are sending people home. We are not meeting the standard of care we have set out for ourselves.”
This was a regrettable situation, but one that would theoretically be addressed within the scope of an emergency step plan, or surge overflow plan. Not only are COVID-positive community members potentially not being treated in hospital due to lack of beds and/or equipment, but non-COVID medical appointments are being canceled or postponed, and non-COVID emergencies are also potentially unable to adequately be addressed for this same reason. The surge in unvaccinated COVID-19 cases is too much for the hospital capacity to bear.
One interviewed employee exclaimed in frustration, “Right now it feels like the wild wild West and people can just do what they want to do. And that’s not OK. This is a hospital! There has to be structure and there has to be plans, and we can’t just keep moving in crisis mode. This is not working.” They went on to describe the influx of COVID patients, and which departments are housing and caring for them. COVID patients are not only in the ICU, they are on the Med-Surg level, also in the progressive care unit, and in the relatively new Intermediate Care Unit (IMCU).
A HOSPITAL CONFORMED TO COVID CARE
Describing how a normal, non-negative pressure hospital room is converted in to a room suitable to meet CAl-OSHA standards for protections when dealing with highly infectious aerosolized disease, one staff member explained, “Basically, what they do when they need to set up a Covid room…[I]f they don’t have one already available- engineering will come in and will seal off the vents that go back into the main hospital. They will open the window fully and attach a plywood wall in the window, and then attach the HEPA vent, and the filtration system is put out the window.”

In each COVID-19 Modified room, a $1,200 HEPA negative airflow machine is configured with attached ducting directed out the window, usually from a second floor window in order to decontaminate the room.
In a challenging setting, nurses and aides must do what they can with what they have, as staff have adapted to the new, modified work space. “They have these big box filters…[I]t’s filtering the air and they have the window sealed off with the tube going out the window. It’s not a true negative pressure room, but they have a filter in there. Engineering comes in, and they do a great job.”
Another staff member expressed confidence in the team effort to provide safe care, saying, “Engineering is good. They check every room that has regular negative pressure on a regular basis to make sure that the negative airflow is intact.”
In regard to the organization of the high-acuity COVID-19 patients throughout the hospital’s sprawling departments, there were some concerns among staff. One veteran caregiver explained, “Ideally, it is clear that you would want to cohort [group] these patients.”
With many years of experience treating very ill patients with a variety of serious ailments, this expert explained that the industry’s best practices dictate how to care for patients in a hospital setting. “You would want to have one nurse focusing on those Covid-positive patients, whether it be in ICU or a Respiratory Care Unit, Or in the intermediate care unit. That would be best practice because you were working with a highly infectious disease.”
Aspects of care considered with best practices include patient isolation in a negative pressure room, specialized care from the same caregiver in order to limit the exposure to the patients, accompanied by required ventilation and adequate protective measures including PPE for all staff.
Keeping all the COVID patients in one area of the hospital, isolated from the rest of the hospital and the patients staying there, is likely not possible without reorganizing high acuity care units across the hospital campus. Instead of arranging the COVID-19 hospitalizations all together, as a cohort, staff are having to simply put the patients “wherever there’s an available room.”
Seeming resigned to the inevitability of the surge, the staff member told us, “It is so much easier for the hospital to get the patients out of the emergency department if you can just put them wherever there is an empty room.”
One reason there is concern regarding where and how a COVID-19 patient is housed relates to the containment of the aerosolized particles that are floating around in the patient’s hospital room. Typically when a patient like this is hospitalized, they are in a negative pressure room, with an adjoining room for a barrier from the common areas outside the hospital room. With these modified rooms, not all of them have this feature – similar to when entering a dark room, an anteroom is a like a waiting room which ensures a safe airflow buffer zone between the controlled pressurized space and an unclean area, called the hot zone where viral particles are assumed to be present.
“Now that we are putting them in the places that do not have an anteroom, anytime you open the door to that room, you get a little bit of backflow into the hall or whatever, so that is what we call a warm zone,” one staff member told us. “So that’s another negative effect of having them spread throughout the hospital and not just in the respiratory care unit or in rooms that specifically have anterooms.”
This issue is not pervasive, but has raised concerns.
In order to create a safe air flow in the RCU area, doors are positioned to maintain a certain directional air flow in the hallway outside COVID rooms. “They used to have a loose plastic sheeting up and everything and they have since taken that down,” a staff member told us. “So on one side of the hallway they have the doors permanently closed and then on the other side of the hallway one door is open for ventilation. So, when you walk through that door, all the patient doors are closed so it’s just the main hallway you’re walking into.”
However, in some spaces in the hospital, this is not completely possible to achieve, and so there are a few areas that staff are aware that may contain airborne particles. “In places where there is no anti-room and you’re directly accessing the patient’s hot zone, it creates what they call a temporary warm zone in the hallway,” one explained.
Ideally, the air flow space used to treat this level of infection – same as they would if they had an active case of Measles, Tuberculosis or Smallpox – is controlled enough that ‘warm zones’ are mitigated as much as possible toward being ‘cool zones’ where there is little to zero airborne particle of the virus present.
A COMPLEX DOCUMENT FOR EMERGENCIES
When we asked Providence St. Joseph Hospital in Eureka’s Press Communications Director Christian Hill where we might find information regarding emergency overflow or surge plan as it relates to the pandemic, we were told, “It is a complex document that isn’t intended for the public.”
Several employees of the Hospital specifically asked for information on this topic, because it is not available to them, either. California hospitals are required to have a contingency plan for emergency purposes, such as a viral pandemic.
In California, the Department Of Public Health sets standards and regulations for how public hospitals are run, particularly during emergencies such surge events and crisis situations which cause resources to have to be triaged. According to COVID-19: Crisis Care — Resources for California Hospitals, “Notification Requirements” specifically note that AFL 20-91 adds several new notification requirements, including the following: “All facilities must notify their local CDPH district office and local public health department via email that they have adopted and publicly posted (including a link to the posting) one of the following: their own crisis care continuum guidelines, another facility’s guidelines, or the state’s California Crisis Care Continuum Guidelines.”
While we have yet to discover this “publicly posted” hospital emergency surge contingency plan or any other EOP, nor have we been conveniently directed to it by Hill – we cannot confirm it does not exist. We can, however, confirm that local healthcare workers and their respective Union representatives have not been able to acquire this information either, not for a lack of trying.
The document further specifically mandates, “Facilities that need to implement crisis care, including triage of critical care resources, must notify their local public health department and local CDPH district office via email and phone call immediately when initiating crisis care to ensure the state is aware of conditions at the facility.”
This is a directive meant to inform Public Health, so that CDPH in local jurisdictions is aware and able to respond accordingly, in the interest of public safety. This would start turning the wheels of local public health service announcements, press releases and news inquiries, all aiming to inform the public and mitigate the potential effects of whatever emergency had befallen the local hospital.
To determine when it is appropriate for hospitals to adopt what is considered “crisis care” certain factors are expected to be affecting hospital operations. CDPH offers this example, “[I]f a hospital is providing cot-based care or any intensive care unit (ICU) care is provided outside usual intermediate and pre/post op areas, these are indicators that operations are now into crisis care and should trigger a response action.” The protocol and operational directives regarding how to manage frontline care would be included in what is called an Emergency Operations Plan, sometimes also referred to in the healthcare field as an emergency step plan, and would include how to manage a surge such as in a pandemic.
In regards to seeing an Emergency Operations Plan (EOP) from St. Joseph, we are told that there is a surge plan in place. Dr. Hoffman describes the plan as “really designed to handle more than we are even seeing currently.” He added, “We decided to demobilize the ACS due to predictions around future surges and vaccination rates. We felt confident that we would not need it, that we could handle that potential 80-bed surge then in the hospital.”
According to the CDPH, “principles of crisis care must be integrated into Emergency Operations Plans (EOPs) at all levels of health care.” And, if crisis care does become imminent, including triage of critical care resources, those facilities must “notify their local public health department and local CDPH district office via email and phone call immediately when initiating crisis care to ensure the State is aware of conditions at the facility.”

Triage Tree, part of the Hospital Crisis Tool Kit, can be used to determine the level of care needed in a crisis situation, where resources are being managed carefully due to a surge event or other emergency.
Speaking with nearly a dozen hospital employees, the staffing levels were not the only major concern brought up by disillusioned hospital workers. Most of them reported experiencing a shortage of equipment used for COVID-19 patient respiratory care, and currently, there are no available non-invasive breathing mechanisms left. They are all being used.
So, as one healthcare worker said, “[T]he options for people right now…For COVID patients or anybody experiencing respiratory distress is high flow oxygen or a ventilator so you’re getting intubated with a tube down your throat… with bipap supplies low. Hospitals usually don’t run into all patients in their care requiring a certain equipment item.”
Another caregiver, frequently tasked with care of COVID-19 positive patients, asked, “How is the hospital planning to respond to the lack of equipment? We are out of the most common size of mask used for the noninvasive ventilators. We are not able to get some of the things we need.” This shortage of equipment is further complicated by elective procedures ongoing during the surge, as these require much of the same resources.
CONTINGENCIES FOR COVID CARE
Regarding the reported shortages in equipment, Providence St. Joseph Hospital in Eureka’s Press Communications Director Christian Hill tells us items have been requested, but did not offer specifics. “We have ordered additional equipment and medication to meet the current and future demand,” he explained. “Some has arrived. Others are coming over the next 2 weeks.”
One staff member explained that in the ER, there is a constant struggle to maintain balance, where too few staff members are available for too many incoming emergent needs. “Sometimes the emergency department is so busy people have to wait for the next day to get care.” This employee explains, “Because there’s not enough doctors and nurses – the emergency department only has 20 rooms and a lot of times half of those rooms are occupied with 5150 patients.” (5150 is the name of the Health Code referring to a person who is experiencing mental health issues.)
Elective surgeries that take up acute care resources (like ICU beds) which would otherwise be used for treating COVID patients were not being canceled across the board, according to our sources. Some of these are ongoing according to feedback received from various departments within the hospital, which further stresses the capacity of caregivers to meet the needs of acute care patients like COVID-19 admissions in the ICU or into the Progressive Care Unit, which both house COVID patients. One staff member told us, “So, we’re doing elective surgeries, and we’re sending people home because we don’t have the beds available.”
However, Dr. Hoffman stated on Tuesday that elective surgeries are being cancelled.
The California Nurses Association has taken the position that staffing ratios directly affect patient care in a serious way. The nurses union has lobbied to institute more controls and oversight on staffing procedures for many years, insisting that “allowing hospitals to set staffing levels that are primarily budget driven, while not setting up a system of accountability, has created a threat to patient safety.”
While some caregivers told us they were comfortable with the current level of organization, there were those that felt very uneasy and questioned the protocol. One staff member lamented, saying, “We have covid positive patients in makeshift rooms where we can’t see them from outside the room. It’s all just so unsafe.” While there are efforts by engineering to correct this problem of not being able to oversee a patient apart from donning and doffing to get into the room to check on them, we do not know how soon these adjustments can be accomplished.

COVID-19 customized hospital rooms, with their plywood and circular ducting ventilation in the windows of each, can be seen from the sidewalk at the graceful entrance to the hospital, here, as well as on the opposite side of the building and the adjacent wing above the ER. [Photo by Ryan Hutson]
One element of help came in the unexpected form of cameras fixed on patients in their beds, as an alternative to having a nurse, aid, or bedsitter attending to the patient at the bedside. According to our sources, these are cameras that are being monitored off site for patients who are altered, fall risks, etc., as well as for COVID-19 patients who are situated in a room which has been modified to accommodate them, which may not have a window allowing a caregiver to view the patient from inside the room. These new cameras are called “telesitters”, and are monitored by staff in Texas. The remote viewing staff in Texas will alert the local nurses of any safety issues that they observe via the telesitting camera.

Telesitter camera allows care providers to see what is going on in a patient’s room even when no one is physically present. [Photo provided]
Designed to assist the nurses on duty by keeping an eye on the patient, the room is outfitted with the camera-microphone system which is remotely monitored by a member of staff who will speak to the patient via the device, if needed. A voice from the remote observer directs the patient as needed, in the absence of a caregiver in the room. “Now we have robot cameras watching them,” a staff member described to us. “They have this, like, eyeball camera thing on a stick, and it’s in the room and it’s facing the patient watching them.”
Describing this new and somewhat unusual technology, they explained how it works in practice. “If the patient takes their oxygen off or tries to pull out their leads, and wires that monitor their heart rate and all that stuff, if they start pulling anything or IVs or anything, there’s a voice in the camera that says to them, ‘put your mask back on, put your mask back on’, or they will say, ‘sir or madam, lay down don’t get out of bed’… .”
According to one staff member, they then asked a manager, “What happens if the patient is actually endangering themselves?” and were told that in that scenario, an alarm would sound and that staff would all be expected to “drop what we’re doing with our patients and go run and help.”
While the cameras do offer some level of security in a situation where they may otherwise be totally left to their own solitude, this nurse concluded, “It does not prevent a patient from harming themselves, and because our staffing ratios are so low, who’s to say that we would be able to get to that patient before they were able to harm themselves?”
One frontline caregiver told us, as we wrapped up the interview, “Our community must get vaccinated if they hope to return to some semblance of normalcy. These covid admissions are completely preventable and are taking up beds in our hospital.”
Another told us that the situation is untenable due to sheer frustration and fatigue among caregivers. Many are expressing outright anger at those choosing to remain unvaccinated as the hospital copes with ongoing turmoil. They speculated, having seen for themselves what the ER and ICU staff are struggling with, “People are now becoming incapacitated and extremely ill, we’re hearing about whole [households] being in the ICU or in the hospital seeking treatment for Covid because people made “my freedoms” and “America” you know, that kind of choice based on politics and not on science to not get vaccinated, and are draining every resource while they attempt to survive their choices… .”
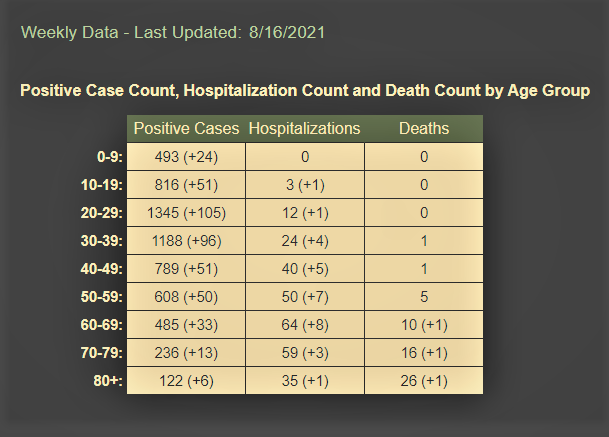
County Dashboard showing local cases, hospitalizations, and deaths cumulatively by age updated August 16 since then there have been multiple deaths including that of a person in their twenties. In coming days, the dashboard data will cease to be provided by the local Health Department and will shift to being provided by the State Health Department.
![]()
![]()
![]()
![]()
Related Posts
